In this post, we will explain how to achieve correct occlusal distance with the One Visit Crown (OVC)
Tooth preparation – how much clearance to leave
When preparing the tooth for the placement of the One Visit Crown, at least 1mm of clearance needs to be allowed in the central fossa and 1.5mm at the cusps and marginal ridges for the OVC to be seated.
The OVC comes with an Occlusal Reduction Guide (ORG), which accurately reflects the size of the cured top-layer of the OVC.
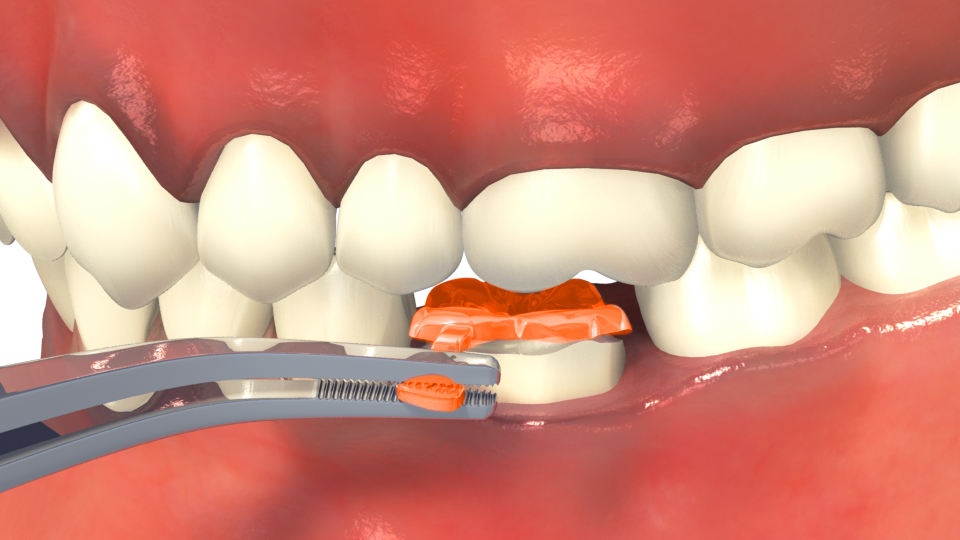
Hold the Occlusal Reduction Guide handle using tweezers, placing it over the prepped tooth, and ask the patient to bite down. Move the Occlusal Reduction Guide gently – it should not be trapped by the occlusion. Please note, this doesn’t mean that it can be pulled completely out – as this is not compatible with the principles of minimal intervention.

If the patient’s bite obstructs the movement of the replica, you know that you need to prep the tooth more. A useful tip is to spray the underside of the Occlusal Reduction Guide with an occlusal spray, to identify where further reduction of the prep is needed after the patient bites down. An example of an occlusal spray you could use is the Bausch Arti-Spray® Occlusion-Spray.
Also check that the Occlusal Reduction Guide hasn’t been tilted due to a plunging opposing cusp – if it is tilted then adjust the opposing dentition as required.
OVC positioning – how to correctly place and align the fissures
 After removing the OVC3 from the black film, reshape the uncured sub-layer to a more conical form. This helps air to escape when pressing the OVC into the matrix band.
After removing the OVC3 from the black film, reshape the uncured sub-layer to a more conical form. This helps air to escape when pressing the OVC into the matrix band.
Take care that no contamination of the uncured sub-layer occurs as a result of the gloves being used intra orally.
Gently depress the OVC to align with the marginal ridges of the neighbouring tooth. If possible, depress it slightly lower than the occlusal plane to minimise occlusal adjustments. Ensure that the OVC is inside the matrix band and not caught on the lip of the band.
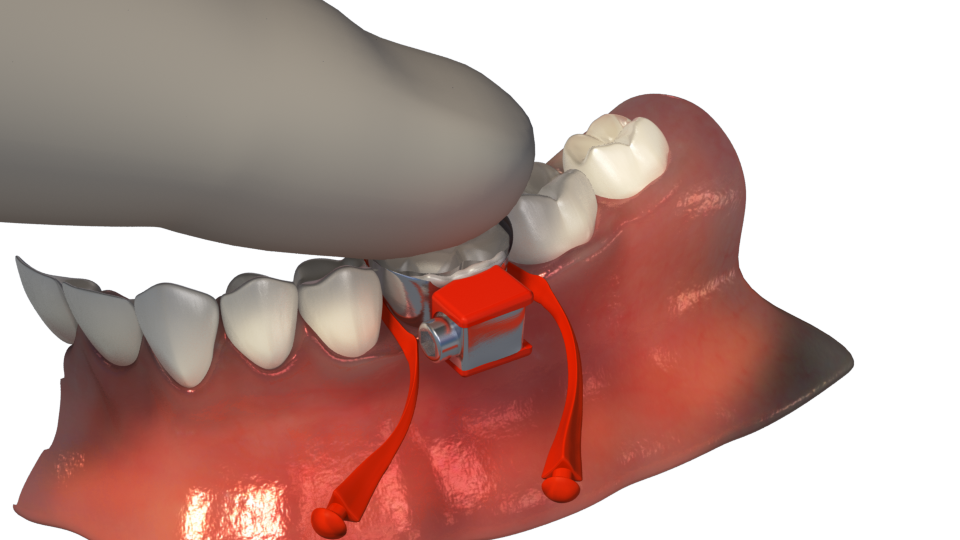
The Occlusal Seating Guide has been custom-made by our lab technician from your patient’s impression. Press the guide down gently to perfectly align the OVC. 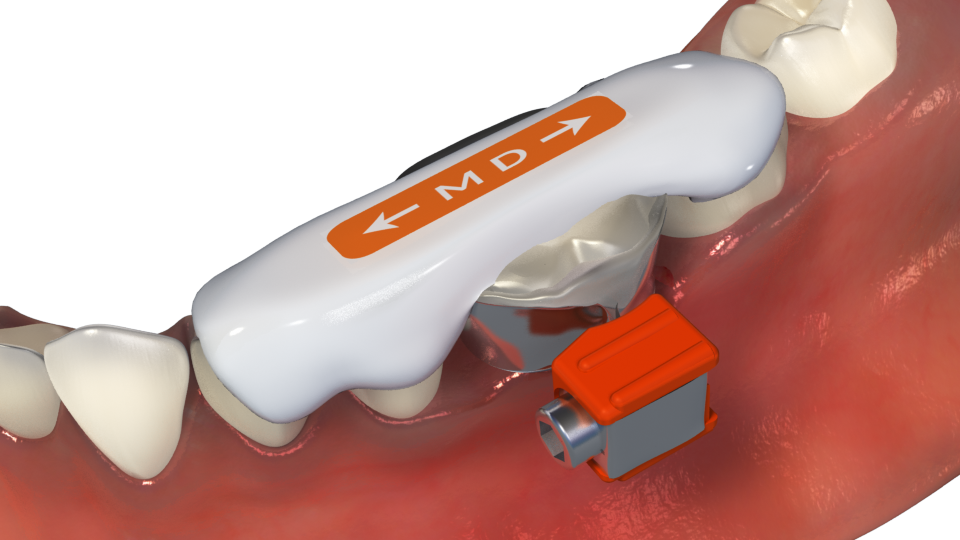
What if the OVC ends up below the occlusal plane?
If the OVC is depressed slightly lower than the marginal ridges of the neighbouring tooth and is therefore marginally out of occlusion, studies have shown that the tooth will naturally erupt back into occlusion over the next couple of weeks[i].
CONCLUSION
If you have any further questions regarding occlusion or the use of the One Visit Crown, email us at info@rhondium.com and one of our product specialists would be happy to help.
Leave us a comment below to let us know how you found this article.
[i] 1.) C. Youngson DDSc, BDS, DRD, MRD, FDS (Rest Dent), RCS(Edin), FDS RCS (Eng, Callum & Manogue PhD, MDSc, BDS, DRD, MRD, FDS RCS (Edin, Michael & Andrew Blance BSc, MSc & L. Craddock, Helen & C. Youngson, Callum & Manogue, Michael & Blance, Andrew. (2007). Occlusal Changes Following Posterior Tooth Loss in Adults. Part 1: A Study of Clinical Parameters Associated with the Extent and Type of Supraeruption in Unopposed Posterior Teeth. Journal of Prosthodontics. 16. 485 – 494. 10.1111/j.1532-849X.2007.00212.x.
https://www.researchgate.net/publication/227605829_Occlusal_Changes_Following_Posterior_Tooth_Loss_in_Adults_Part_1_A_Study_of_Clinical_Parameters_Associated_with_the_Extent_and_Type_of_Supraeruption_in_Unopposed_Posterior_Teeth
2.) L Craddock, H & C Youngson, C. (2004). Verifiable CPD Paper: Eruptive tooth movement — the current state of knowledge. British Dental Journal. 197. 385-391. 10.1038/sj.bdj.4811712.